| Is the pain articular? | | | Is the condition inflammatory? | | | Are there associated signs and symptoms? | | | Acute or Chronic? | | | How many joints are involved? | | | Are joints affected symmetrically or asymmetrically? | | | What type of joints are affected? |
| | Is the pain articular? |
|---|
There are many structures outside of the joint capsule ('periarticular') which may be a source of pain or dysfunction. This creates a clinical picture that can be confused with true articular pathology. Differentiating these is important. Key Point 1: Have the patient point to the site of pain.Correlate the point of maximal tenderness with your knowledge of anatomy. Is the most likely structure involved intra- or extra-articular? Remember, you can be fooled by referred pain (e.g. knee pain that originates from the hip or back). Fibromyalgia is a chronic pain condition characterized by tenderness in the soft tissues (muscle, tendon) that can be confused with arthritis. In this disease, tenderness is often maximal at characteristic sites in the muscles ("trigger points"). Key Point 2: What effect does joint motion have on the patient's symptoms?
In an articular disorder, the patient generally reports pain throughout most of range. You may also notice crepitus which is also suggestive that the pathology is in the joint. Peri-articular or non-articular disorders are not usually associated with a painful range of motion. Peri-articular ligamentous injuries may be associated with pain when the ligament is specifically stressed. |
| Is the condition inflammatory? |
|---|
Arthritis may or may not involve inflammatory changes in the joints. This is an integral element of diagnosis. Key point 1: Symptoms characteristic of inflammation- Joint swelling (effusion)
- Warmth
- Redness (variable; most commonly seen in superficial joints in cases of infection or crystal arthritis)
- Pain (also noted in non-inflammatory joint disorders)
Key Point 2: Morning stiffness.Morning stiffness that lasts at least 60 minutes is a cardinal feature of inflammatory arthritis. Stiffness is also noted after periods of rest. This is termed "gelling". While patients with non-inflammatory arthritis may complain of morning stiffness, it is not prolonged. | | Hands of a child with JRA. Note the swelling of the middle finger PIP. (©iStockphoto.com/JynMeyer) | |
|
|
|
| Are there associated signs and symptoms? |
|---|
Some rheumatological disorders are associated with systemic and/or extra-articular signs and symptoms. Key Point 1: You won't find out if you don't ask.Patients may not realize extra-articular features may be associated with their joint problems. Always include a complete review of systems when assessing a patient with an undiagnosed rheumatologic disorder.Key Point 2: What to look for.- Systemic symptoms - fever, chills, anorexia, lethargy and weight loss often herald infectious or inflammatory arthritides.
- Skin changes - these include dryness, rash, colour change and mucosal ulceration.
- Raynaud's Phenomenon - vascular spasm in the digital arteries causes dramatic colour changes in the hands and feet. Patients may notice changes in a cold environment and described them as turning red, white and blue.
- Altered bowel habit - certain gastrointestinal conditions are associated with autoimmune and post-infectious arthritides. Ask about consistency and frequency of stool as well as whether the patient has noticed mucus or blood.
| | Facial (malar) rash characteristic of SLE (©ACR www.rheumatology.org) | |
|
|
|
| Acute or Chronic? |
|---|
Arthritis is commonly a chronic problem, however some related disorders may be acute and self-limited. This feature is another important clue to diagnosis. Key Point: What is the definition of a chronic arthritis?The condition is considered chronic if it has lasted more than 6 weeks.
| | Chronic inflammation of the small joints in the hand have led to a characteristic RA pattern of deformity (©ACR www.rheumatology.org) | |
|
|
|
| How many joints are involved? |
|---|
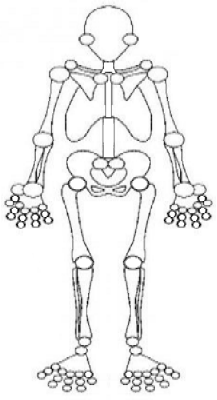
Some diseases characteristically affect one joint (monoarthritis) while others affect many joints (polyarthritis). Key Point 1: Keeping count.Joint diagrams, like the one below, allow precise documentation of the number of "active" joints that a patient is experiencing at a point in time. This is used to diagnose and follow the disease.Key Point 2: Definitions.Monoarthritis: One joint affected.Oligoarthritis: 2 - 4 joints affected. Polyarthritis: 5 or more joints affected. |
| Are joints affected symmetrically or asymmetrically? |
|---|
If more than one joint is affected, it's important to determine if the affected joints are symmetric as certain disorders have characteristic patterns. Key Point 1: Symmetrical arthritic conditions.Rheumatoid arthritis is classically symmetrical. This may also be the case in primary osteoarthritis. | | This patient has primary osteoarthritis affecting all of her DIP joints. ©iStockphoto.com/Rinderart | |
|
|
Key Point 2: Asymmetrical arthritic conditions.Seronegative arthritides and secondary osteoarthritis are commonly asymmetrical. |
| What type of joints are affected? |
|---|
Some diseases preferentially affect the axial skeleton (spine/pelvis); others favour the appendicular joints. The latter can be subcategorized by joint size. Key point 1: When is the axial skeleton involved? Rheumatoid arthritis may affect the cervical spine but usually spares the lumbar spine and pelvis. Disease in these areas is usually associated with osteoarthritis and seronegative conditions.Key point 2: Is a joint considered small or large?Small: MCP, IP, CMCs, PIPs, DIPs, MTPs.Large: Shoulder, elbow, hip, knee, ankle. |
|
|